Welcome to the New Mexico Foodborne Illness Investigation Online Training
This training was designed to accompany the Foodborne Illness Investigation Training Manual developed by the New Mexico Department of Health and the New Mexico Environment Department. This manual defines foodborne illness investigation partner roles and responsibilities, describes investigation procedures, and addresses public education, and corrective measures. Chapters 1 and 2 introduce the preliminary building blocks to an effective response.
Please Note
This online course will take approximately 1 - 2 hours to complete.
Upon completion there will be an assessment.
A passing score of 80% or higher will be necessary to recieve your Certificate of Completion.
Welcome to the New Mexico Foodborne Illness Investigation Training. This training was designed to accompany the Foodborne Illness Investigation Training Manual developed by the New Mexico Department of Health and the New Mexico Environment Department. This manual defines foodborne illness investigation partner roles and responsibilities, describes investigation procedures, and addresses public education and corrective measures. Chapters 1 and 2 introduce the preliminary building blocks to an effective response.
The purpose of this manual is to provide guidance for prompt detection of and response to foodborne illness outbreaks in New Mexico, recognizing that a successful foodborne illness outbreak investigation requires collaboration between partners from the disciplines of epidemiology, environmental health, food science, and microbiology. The most important reason to investigate foodborne illness cases is to identify the cause of disease and how it might be further spread so that appropriate actions can be taken to prevent additional illness.
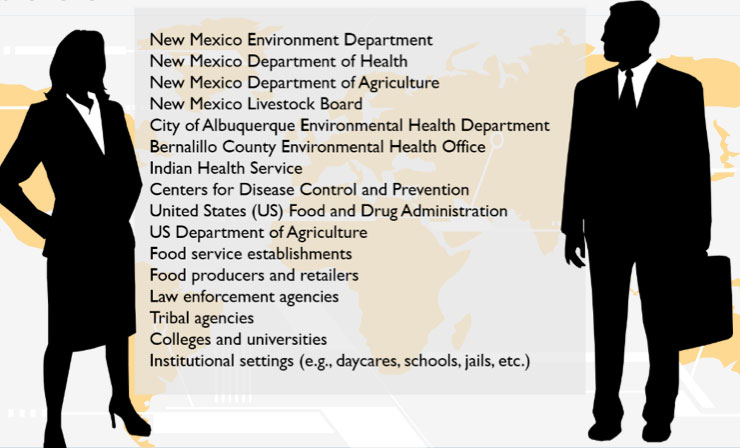
Depending on the nature and scope, foodborne illness investigations in New Mexico can involve government agencies at the federal, state and local levels, as well as private and community partners. Contact information for many potential partners is in Chapter 10.1 of your manual.
Data on individuals collected during a foodborne illness investigation is confidential under New Mexico law and New Mexico Department of Health (NMDOH) policy. For this reason, data collection on individuals is the responsibility of state or local public health officials and should not be delegated. When data collection instruments are distributed to persons involved in an investigation via a third party, the completed original instruments should be returned directly to the state or local public health officials without copies being made and without passing through the third party, except when the third party is obligated by law to maintain patient confidentiality.
Knowledge Check
When it is necessary to provide patient specific information in a written report...
...patients should be identified using a pseudonym
Correct!
...all entities involved sign a confidentiality contract
The rest of this training module provides a brief overview of the epidemiology of foodborne illness. This information has been adapted from the CDC’s Food Safety home page. For more information, follow the link provided here and in Chapter 2 of your manual.
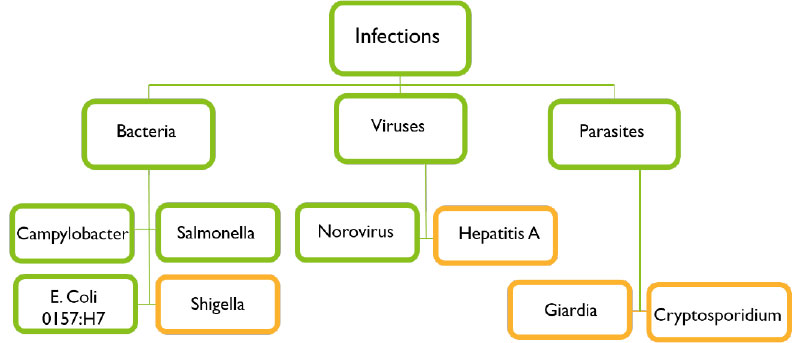
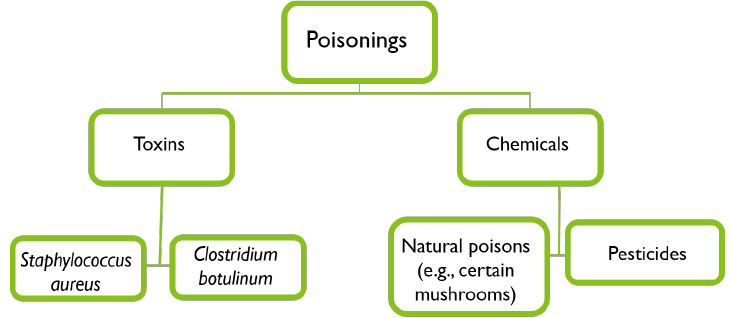
More than 250 different foodborne illnesses have been described. Many of these illnesses are infections, caused by a variety of bacteria, viruses, and parasites that can be transmitted through food. Other illnesses are poisonings, caused by toxins or chemicals contaminating food.
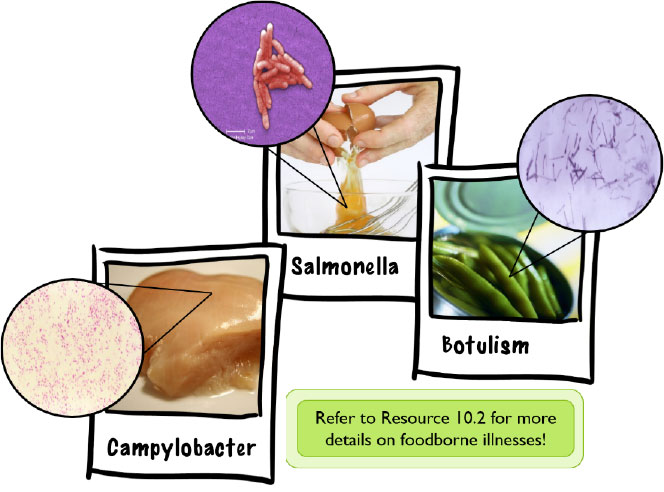
The most commonly recognized foodborne infections are those caused by the bacteria Campylobacter, Salmonella, and Escherichia coli O157:H7, and by a group of viruses called calicivirus, with the most frequent being norovirus. Some common infections are occasionally foodborne, even though they are usually transmitted by other routes. These are illustrated below in orange and include infections caused by Shigella, Hepatitis A, and the parasites Giardia and Cryptosporidium.
Other toxins and poisonous chemicals can cause foodborne illness. People can become ill if a pesticide is inadvertently added to a food, or if naturally poisonous substances are used to prepare a meal, such as poisonous mushrooms or certain reef fishes. Botulism, which is caused by the botulinum toxin is considered a medical emergency as untreated cases may lead to paralysis and death.
Foodborne illness agents may be transmitted in more than one way, such as person-to-person or animal-to-person. Foodborne illness outbreaks due to Shigella, Staphylococcus aureus, hepatitis A and norovirus are generally caused by contamination of uncooked or cooled foods by an infected food handler. Foodborne illness agents from animal-derived foods like eggs or meat can cross-contaminate raw foods through cooking utensils, the hands of food handlers, or food preparation surfaces. Pathogens with an animal reservoir may also be transmitted directly through food, such as ground beef contaminated with E. coli or eggs infected with Salmonella. Norovirus can be transmitted via aerosolized vomitus and from contaminated surfaces. Clostridium perfringens and Bacillus cereus are ubiquitous in the environment and outbreaks caused by these agents generally result from holding food at a temperature that allows the organism to proliferate.
Foodborne infections are usually diagnosed by specific laboratory tests that identify the causative organism. Bacteria such as Campylobacter, Salmonella, and E. coli O157 are best identified by culturing stool samples although there are other rapid tests available. Parasites like Giardia and Cryptosporidium are identified by testing stool with specific enzyme immunoassay tests. Viruses are more difficult to detect and are usually identified by testing stool samples by polymerase chain reaction that identifies the specific virus present. Foodborne illnesses caused by toxins or poisonous chemicals are usually diagnosed by the presence of specific signs and symptoms in the ill person.
Foodborne illnesses require different treatments depending on the symptoms they cause. Illnesses that involve primarily diarrhea or vomiting may require only adequate hydration. Antibiotics are usually not recommended for most foodborne illnesses and healthy people typically recover without medical treatment. Pregnant women, the elderly, very young children, and those with weakened immune systems are more likely to develop serious illness and may need special treatment.
Hazard Analysis and Critical Control Points (HACCP)
Hazard Analysis and Critical Control Points (HACCP) is a system of preventive controls that is the most effective way to insure that food products are safe. This system was developed for the space program over 30 years ago. HACCP focuses on preventing, controlling, or eliminating hazards that could cause foodborne illnesses by applying science-based controls, from raw materials to finished products. It has seven principles, each of which must be backed by sound scientific knowledge, such as published microbiological studies on time and temperature factors for controlling foodborne pathogens.
Analyze Hazards
Identify potential hazards and measures to control those hazards. For example the hazard could be:
Biological (e.g., bacterium)
Chemical (e.g., toxins)
Physical (e.g., metal fragments)
Identify CCPs
Critical Control Points: points in a food’s production at which the potential hazard can be controlled or eliminated. For Example:
Cooking
Cooling
Packaging
Metal Detection
Establish preventative measures
Include critical limits for each control point. For Example:
Set the minimum cooking time required to ensure the elimination of any harmful bacteria
or viruses
Establish monitoring procedure
Monitor CCPs. For Example:
Determine how and by whom cooking temperature should be monitored
Establish corrective actions
Implement when monitoring shows that a critical limit has not been met. For Example:
Reprocess or dispose of food if it does not reach minimum cooking temperature
Establish confirmatory procedures
Verify that the system is working properly For Example:
Test time-and-temperature recording devices to ensure that a cooking unit is working well
When conducting an environmental inspection as part of a foodborne illness investigation, the investigator should apply HACCP principles to focus on those food handling procedures and processes that pose the greatest potential for foodborne illness. Check whether the associated critical care points were achieved and if not, why they were not achieved.
This module provided a brief introduction to the investigation of foodborne illness outbreaks. With this information, you will be able to continue on to the following modules with a greater understanding of the purpose of outbreak investigations as well as the epidemiology of foodborne disease. Continue to Module 2 to learn about the roles and responsibilities of the partners in the investigation team.
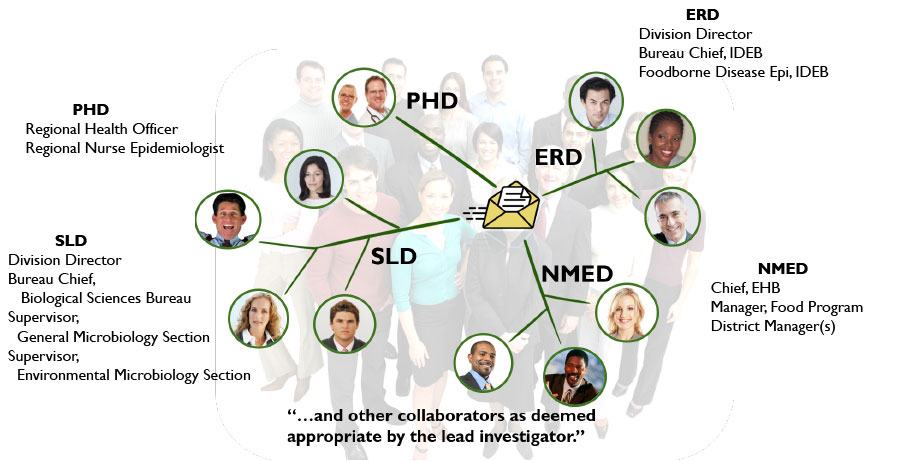
The investigation of a foodborne illness outbreak requires the participation of several organizations on the federal, state, and local levels. In this module you will learn and understand the roles and responsibilities associated with two major investigation participants, the New Mexico Department of Health and the New Mexico Environment Department. For most outbreaks, the majority of investigation and follow-up will be completed by these two state departments.
The New Mexico Department of Health has legal authority to protect the public’s health and is responsible for directing and coordinating investigations of potential foodborne illness. During a foodborne illness outbreak, three NMDOH entities are usually represented as part of the investigation team, the Public Health Division, the Infectious Disease Epidemiology Bureau (part of the Epidemiology and Response Division), and the Scientific Laboratory Division.
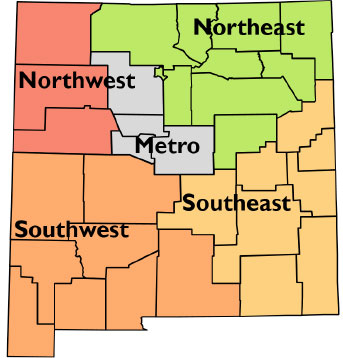
There are five regions in the NMDOH Public Health Division (PHD) and each region encompasses a number of local public health offices (PHO). Within their respective jurisdictions, local and regional PHD staff members have primary responsibility for the following foodborne illness investigation activities. The map shows all five of the public health regions.
Investigation
Connect NMDOH and the community
Coordinate response with IDEB
Ensure involvement of appropriate PHO(s)
Investigate illness reports
Gather descriptive epidemiologic information
Develop patient/food handler questionnaires
Administer patient/food handler interviews
Specimen Collection
Coordinate with IDEB, NMED, and SLD
Collect, package, and ship food/clinical specimens
Data on individuals collected during a foodborne illness investigation is confidential under New Mexico law and New Mexico Department of Health (NMDOH) policy. For this reason, data collection on individuals is the responsibility of state or local public health officials and should not be delegated. When data collection instruments are distributed to persons involved in an investigation via a third party, the completed original instruments should be returned directly to the state or local public health officials without copies being made and without passing through the third party, except when the third party is obligated by law to maintain patient confidentiality.
Investigation
Coordinate investigations
Ensure involvement of appropriate federal, state, and local agencies
Determine nature and extent of investigation
Gather descriptive epidemiologic information
Investigate reports of illness
Develop patient/food handler questionnaires
Administer and provide quality assurance for patient/food handler interviews
Specimen Collection
Coordinate with PHD, NMED and SLD
Ensure proper specimen collection, handling, and testing.
Data Analysis
Perform statistical analyses to test hypotheses
Reporting results
Report results of laboratory testing to investigation partners
Report select conditions to CDC
Develop public notifications
Prepare final written summary report
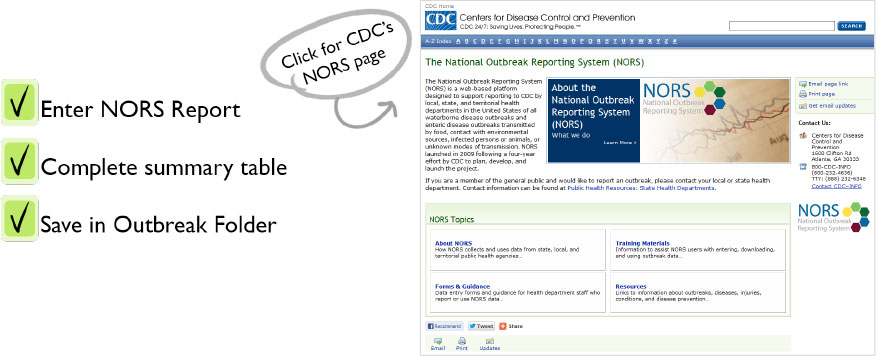
Complete NORS report
(National Outbreak Reporting System)
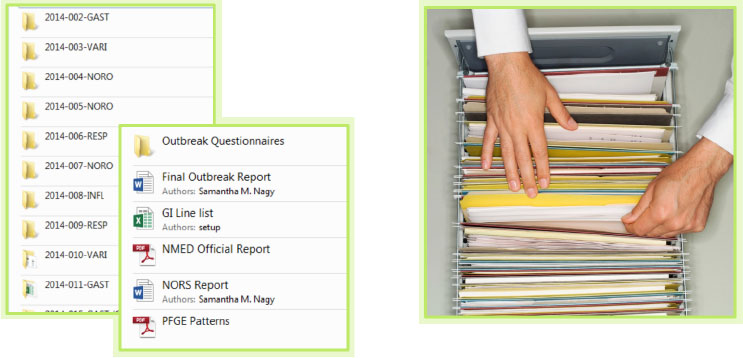
Archive all investigation documentation
E.g., notes, line lists, questionnaire, interview data, laboratory results, written reports.
Control measures
Collaborate with partners to recommend control measures
The NMDOH Scientific Laboratory Division (SLD) is the public health reference laboratory for New Mexico. Hospitals and other laboratories in New Mexico routinely send clinical, environmental, and food specimens to SLD for identification, confirmation, serotyping, and molecular subtyping. SLD is the only Laboratory Response Network (LRN) facility in the state and has the capability to provide emergency response work for bioterrorism events as well as for foodborne illness outbreaks. SLD has primary responsibility for the following foodborne illness investigation activities.
Specimen Collection
Provide guidance and consultation regarding proper specimen handling and transport.
Testing
Provide microbiological testing of clinical, food, and other environmental specimens
Coordinate with other state and federal reference laboratories
Send specimen to CDC for confirmation
Reporting Results
Report laboratory test results to PHD, IDEB, NMED, and private submitters and ensure involvement of all appropriate local agencies
The New Mexico Environment Department (NMED) has legal jurisdiction over regulated food facilities and related activities. Facility (as used in this manual) can mean a regulated food service or food processor facility, any facility regulated under the Food Act, a public water supply, public swimming pool, spa or bath, or any other entity regulated under the Environmental Quality Improvement Act. (EHB = Environmental Health Bureau)
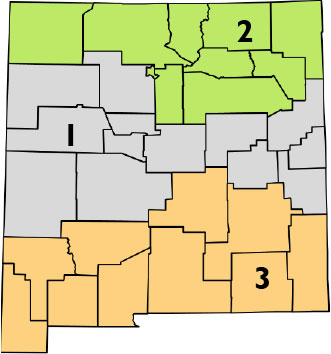
There are three districts in the NMED Environmental Health Bureau (EHB) and each district encompasses a number of local field offices. Within their respective jurisdictions, EHB staff members have primary responsibility for the following foodborne illness investigation activities.
Investigation
Perform facility inspections
Review food handling practices
Generate list of foods and beverages potentially associated with the illness
Administer food handler questionnaires
Specimen Collection
Coordinate with IDEB, NMED, and SLD
Collect, package, and ship food/environmental specimens
Ensure chain of custody is followed
Control measures
Implement legal administrative actions
E.g., permit suspension, facility closure
Reporting results
Develop public notifications
Summarize inspection findings in an official report and share with IDEB for archiving
This module provided a brief introduction to the investigation of foodborne illness outbreaks. With this information, you will be able to continue on to the following modules with a greater understanding of the purpose of outbreak investigations as well as the epidemiology of foodborne disease. Continue to the next module to learn about the roles and responsibilities of the partners in the investigation team.
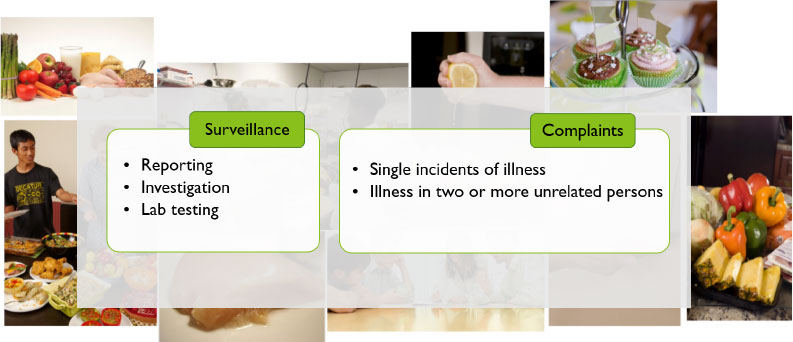
In this module you learn the various ways our agencies can detect a foodborne illness outbreak, namely, though routine surveillance for notifiable foodborne illnesses, individual foodborne illness complaints, and reports of gastrointestinal illness by health care providers, schools, daycares, and other institutions. Information from this module is taken from Chapter 4 in your manual and references useful templates in Chapter 11.
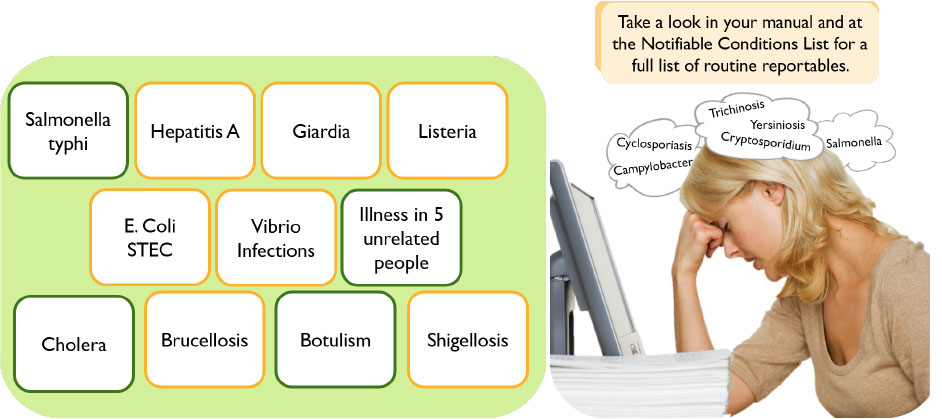
Routine surveillance for foodborne illness in New Mexico consists of the systematic collection, analysis, interpretation, and dissemination of data on persons with confirmed or suspected notifiable foodborne illness. Timely and complete investigations remain crucial to identifying clusters and outbreaks of foodborne illness.
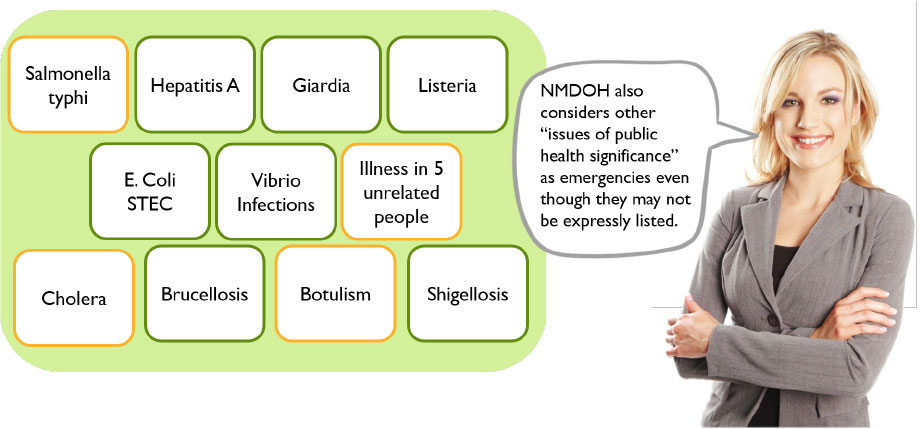
These diseases are commonly transmitted through food and included on the New Mexico notifiable conditions list. See section 10.5 for the full notifiable conditions list.
[Click on the conditions you think are emergency notifiable.]
Salmonella typhi
Yes! This should be reported to IDEB immediately.
Hepatitis A
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Giardia
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Listeria
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
E. Coli STEC
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Vibrio Infections
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Illness in 5 unrelated people
Yes! This should be reported to IDEB immediately.
Cholera
Yes! This should be reported to IDEB immediately.
Brucellosis
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Botulism
Yes! This should be reported to IDEB immediately.
Shigellosis
I'm sorry, this condition is not an emergency, but it should be reported to IDEB within 24 hours.
Each report of a notifiable foodborne illness is referred to a local or regional public health office for investigation. Patients are interviewed with a standardized questionnaire (Template 11.1.1) to collect information on risk factors. Regional and Infectious Disease Epidemiology Bureau epidemiologists review results of those investigations to identify important exposures.
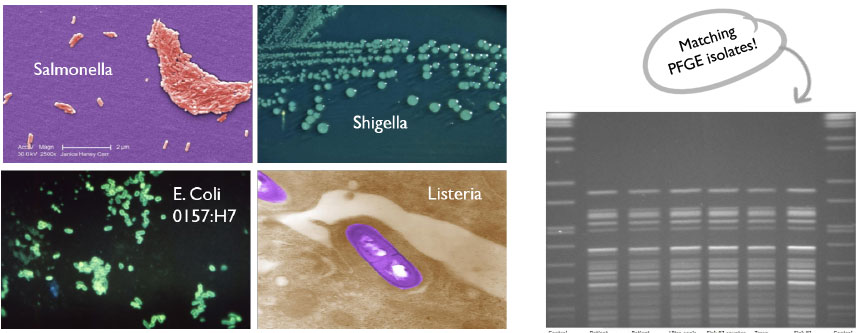
Another key component of routine surveillance is laboratory testing. Bacterial isolates of Salmonella, Shigella, Listeria, and Shiga toxin-producing E. coli (STEC) are required to be submitted to SLD for serotyping and DNA fingerprinting using pulsed-field gel electrophoresis (PFGE). Infectious Disease Epidemiology Bureau epidemiologists review serotype and DNA fingerprinting results to identify clusters of potentially related organisms.
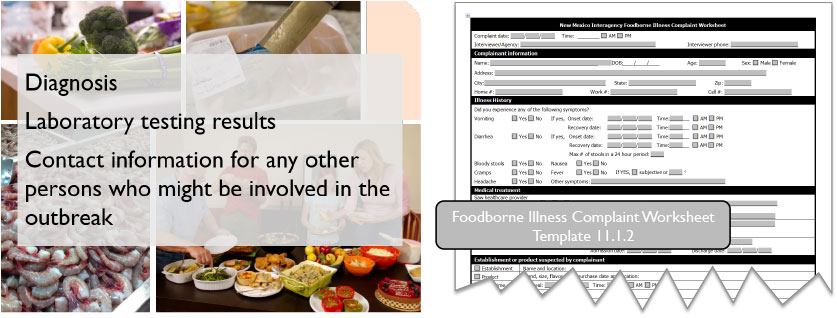
Individual foodborne illness complaints can lead to the detection of foodborne illness outbreaks. Foodborne illness complaints may be received by a number of state and local government agencies. All potential foodborne illness complaints without laboratory confirmation received by NMDOH or NMED personnel should be documented using the Foodborne Illness Complaint Worksheet (Template 11.1.2) and forwarded to the appropriate agency as will be described in the following slides.
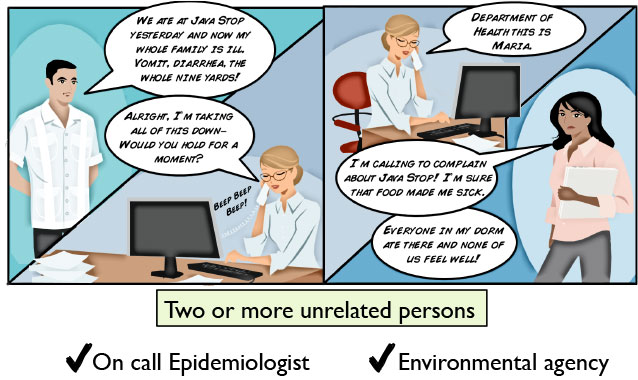
If you receive a complaint involving two or more unrelated persons, that is, people from different households or otherwise unrelated, who develop similar illness at about the same time after sharing a common food or meal, notify immediately by phone and fax completed worksheet to the ERD on-call Epidemiologist and the environmental health regulatory agency with jurisdiction over implicated food facility. Depending on where the offense took place, this could be the Environment Department’s Environmental Health Bureau Field Office, the City of Albuquerque Environmental Health Department, the Bernalillo County Environmental Health Office, or Indian Health Service’s Environmental Health Division.
If you receive a complaint involving a single ill person or two or more persons with similar illness from the same household (or otherwise related) fax completed worksheet within one working day to the environmental health regulatory agency with jurisdiction over implicated food facility. Again, this could be an NMED EHB Field Office, the City of Albuquerque Environmental Health Department, Bernalillo County Environmental Health Office, or IHS Environmental Health depending on the location of the facility. Also, fax the worksheet to the Foodborne Disease Epidemiologist at IDEB and the regional or local public health office, if prior arrangement has been made with IDEB.
In this module you learned the key methods used to detect a foodborne illness outbreak. All of these methods are essential to ensuring the safety of the public. In the following modules you will learn how to proceed with the investigation after the outbreak is detected.
Module 3 discussed how to detect a foodborne illness outbreak. In this module, you will learn and understand the basic steps that should be followed when conducting an epidemiologic investigation of a potential foodborne illness outbreak. The material in this module references Chapter 5 in the Foodborne Illness Investigation Manual as well as resources in Chapter 10 and templates in Chapter 11.
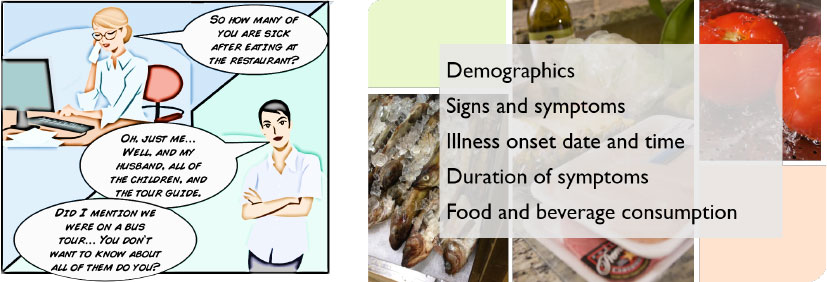
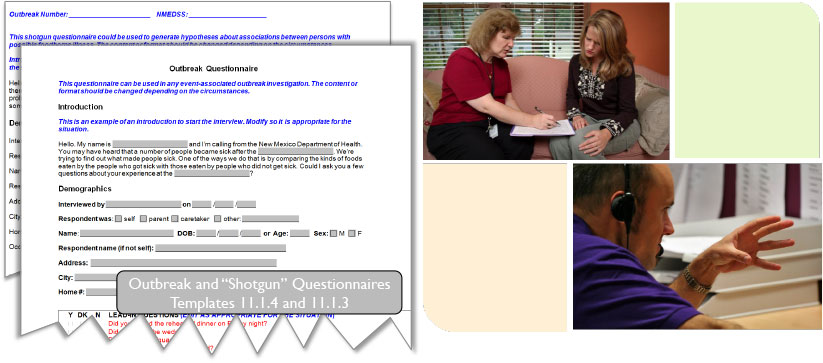
Upon being notified of a potential foodborne illness outbreak, it is important to gather information that will aid in determining the level of investigation required. For individual complaints of possible foodborne illness, use the Foodborne Illness Complaint Worksheet. For clusters of possible foodborne illness associated with a common exposure, use the Foodborne Illness Hypothesis Generating (“Shotgun”) Questionnaire or Outbreak Questionnaire templates to generate a questionnaire. All of these resources can be found in template form in your Foodborne Illness Investigation Manual.
Regardless of the method you use to gather information, ensure that the following information is acquired:
Demographics - including name, address, telephone number, age, gender, and other relevant information such as occupation, school or daycare
Signs and symptoms- including nausea, vomiting, diarrhea, bloody diarrhea, fever, abdominal cramps, muscle aches, chills, unusual fatigue, headache and any other signs or symptoms present
Illness onset date and time
Duration of symptoms
And food and beverage consumption history for at least 72 hours prior to illness onset.
In addition, document whether or not medical care was sought, medical diagnosis, and any laboratory testing results. It is also important to record contact information for any other persons, ill or not ill, who might be involved in the outbreak.
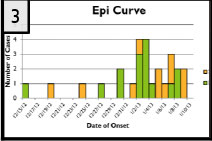
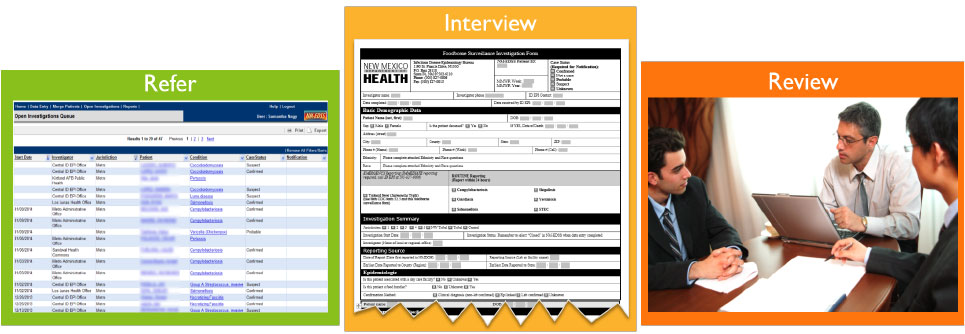
[Click or Hover your mouse on the images below to interact with them]
Based on the information collected, determine whether or not a foodborne illness outbreak exists and, if so, the level of investigation required. Consider the following questions:
Are there two or more unrelated persons who developed similar illness after sharing a common food or meal?
Are the clinical signs and symptoms, dates of illness onset, duration of illness and incubation period consistent with a foodborne disease agent?
Is the number of ill persons higher than would normally be expected in this group of people and in the population as a whole?
Have other organizations or agencies received reports of potentially associated illness?
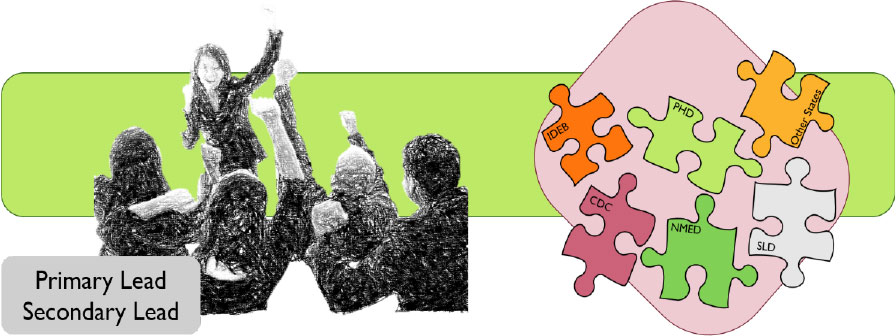
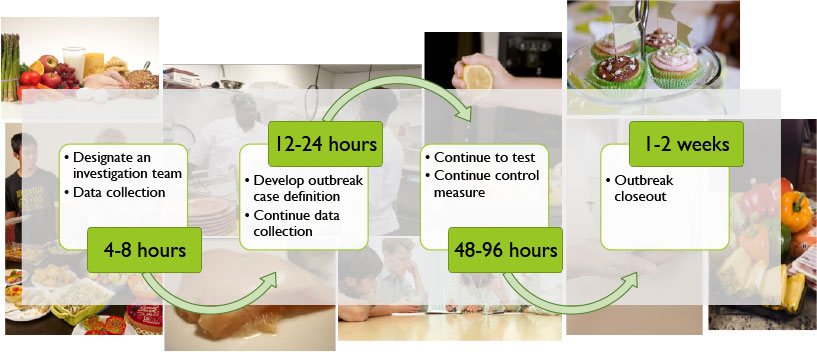
It is important that an investigation team is assigned to each outbreak, and that primary and secondary lead investigators are assigned to each team. Depending on the situation, the investigation team could include representatives from various divisions of the Department of Health, local and regional Environment Department offices, and other governmental agencies. Daily verbal and written communication between investigation team members should be maintained throughout the investigation. Upon report of a potential outbreak, it is unlikely that assembling a large multiagency team will be necessary right away. The size and breadth of the team should match the size and scope of the outbreak and can grow or shrink as the outbreak evolves.
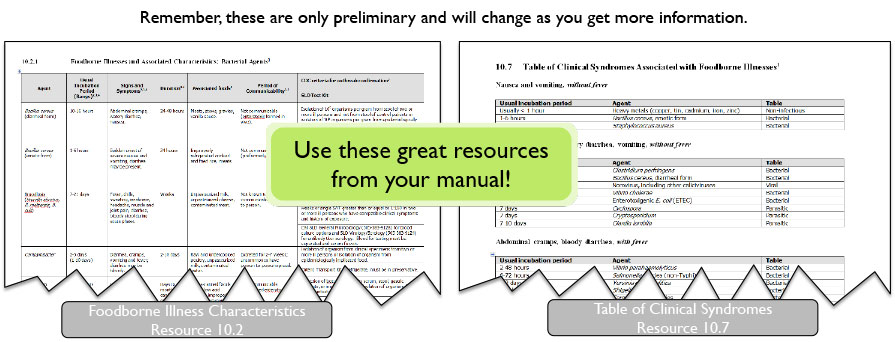
Following preliminary information gathering, the next step is to hypothesize the most likely foodborne pathogens based on signs, symptoms, dates of illness onset, duration and incubation period.
Another important element to develop is the preliminary case definition, which should include person, place, and time.
The type of analysis is determined by many factors including the amount of information available and the level of involvement required. In fact, multiple strategies of analysis may be employed if necessary.
Descriptive
A basic summary that identifies patterns and trends in a situation and helps in generating hypotheses on which further investigation may be based.
Case-control
Compares patients who have a disease (cases) with patients who do not have the disease (controls), and looks back to see how often the exposure to a certain food is reported by each group to determine the relation between the food and the disease.
Case-Case
Compares individual cases associated with an outbreak to sporadic cases within the population.
Obtain as complete a list as possible of all potentially exposed persons and conduct case finding by means appropriate to the investigation. For example, talking to cases, contacting area health care providers, obtaining restaurant reservation lists and/or credit card receipts, obtaining event guest lists or issuing a press release. Also consider other groups that may have been affected, such as other parties catered by the same food service establishment or other groups attending the same gathering. Coordinate with the Environment Department to obtain a menu from the food service establishment or other list of foods as appropriate. Use the list of foods and beverages for hypothesis generation and questionnaire development.
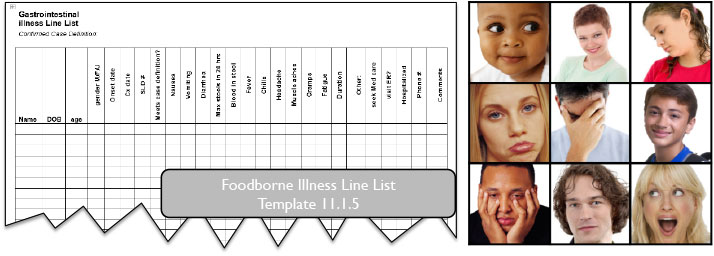
As cases are identified, document information in a line list using the Foodborne Illness Line List Template. The line list should contain, at minimum, demographics, symptom profile, illness onset date and time, case definition classification, and laboratory testing results. Finally, establish a surveillance system for identifying subsequent cases and assessing ongoing transmission as appropriate to the investigation.
A standardized questionnaire, which may be modified if necessary, can be used to interview as many exposed persons, both ill and well, as possible. The Foodborne Illness Shotgun Questionnaire or Outbreak Questionnaire templates may be used as a starting point for questionnaire development. Begin interviews as soon as possible after the first case is identified in order to obtain the most reliable data. Once data are collected, use an excel spreadsheet to record questionnaire data in a timely fashion for analysis. Establish a system for identifying subsequent cases and assessing ongoing transmission as appropriate to the investigation and continue to record data as new information is received.
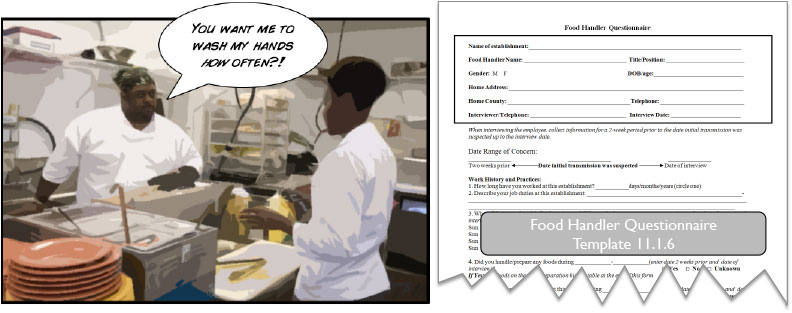
Food handler interviews should be coordinated with the Environment Department (NMED). Using a standardized questionnaire, interview all food handlers, regardless of job duties or shifts worked. The Food Handler Questionnaire may be used or it may be modified. At a minimum, the questionnaire should include the following information:
Work history or schedule
Job tasks and responsibilities
Illness history
Recent illness among household members
Other establishments where employed
Food service establishment employee absentee records should also be reviewed in collaboration with NMED. Like with data collected from exposed individuals, data acquired from food handlers should be recorded in a timely manner.
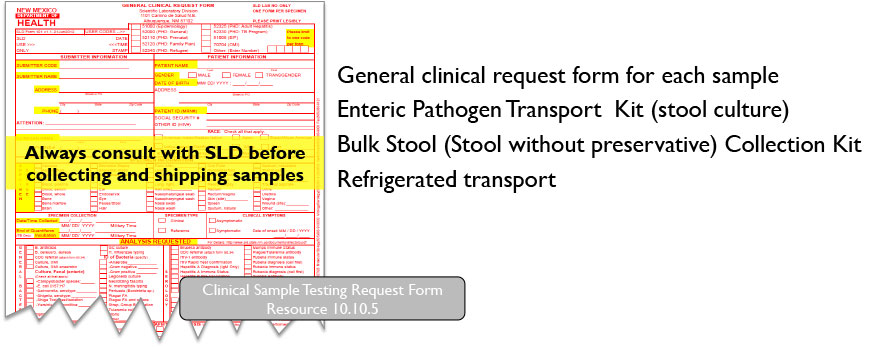
The nature of the foodborne illness outbreak will determine what testing should be done at the Scientific Laboratory Division (SLD). Consult with the on-call epidemiologist from the Infectious Disease Epidemiology Bureau (IDEB) to determine appropriate testing. SLD requires approval from an infectious disease epidemiologist prior to testing outbreak related specimens. If no test kits are readily available they may be ordered from the lab. If the patient will be collecting the stool specimen at home, create a take-home kit with the necessary components and instructions. After the specimen has been collected, ensure the patient’s full name and date and time of specimen collection are written on the sample container or tube.
Specimens should be collected as soon as possible after onset of symptoms to increase the likelihood of identifying a causative pathogen.
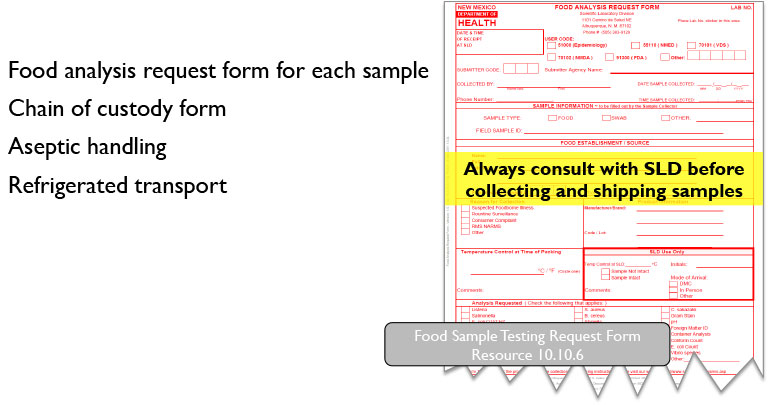
Coordinate with Scientific Laboratory Division (SLD) and the Environment Department (NMED) on proper food specimen collection and handling. If cases have food specimens available in the form of leftovers or “doggie bags”, request that they be saved and refrigerated in the event they are needed for testing.
Before submitting any food samples for analysis, please contact the Environmental Microbiology lab at SLD for guidance regarding the sample collection and testing. Always use the chain of custody form.
Proper collection, identification, and the shipment of a sufficient amount of sample material to the laboratory is essential. If the samples are not properly collected, are mishandled during transport to the lab, or are not representative of the sampled lot, then there is an increased likelihood that laboratory results will be meaningless.
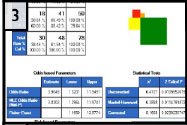
Perform the following analyses as appropriate using Excel or by importing the line list into Epi Info7 and using the analytic tools. This information will be used to finalize a case definition and complete the final report.
Control measures and prevention activities should be recommended based on the characteristics of the outbreak including etiologic agent, implicated food items, environmental investigation findings and facility setting. Depending on the etiologic agent, isolation and work or daycare exclusion criteria may apply. If necessary, the Environment Department will coordinate recall and trackback activities with Infectious Disease Epidemiology Bureau partners.
Prepare a final written report summarizing the epidemiologic investigation within two weeks of investigation completion. Fill in the template and any other necessary reporting forms. Be sure to distribute the report to all contributing parties. If appropriate, conduct an evaluation of the investigation process detailing key points and lessons learned from the investigation.
In this module, you learned the basic steps of an epidemiologic investigation. Remember, though the material in this module is typical, there may be exceptions depending on the specifics of an investigation.
In this module, you will learn the basic steps to conducting an environmental investigation of a foodborne illness outbreak. Remember, an environmental investigation is not a routine inspection, but an inspection triggered by an outbreak or a food contamination incident. The purpose of the investigation is to determine how the environment contributed to the introduction and transmission of pathogens or other hazards that caused illness or contamination. The material in this module references Chapter 5 in the Foodborne Illness Investigation Manual as well as resources in Chapter 10 and Chapter 11.
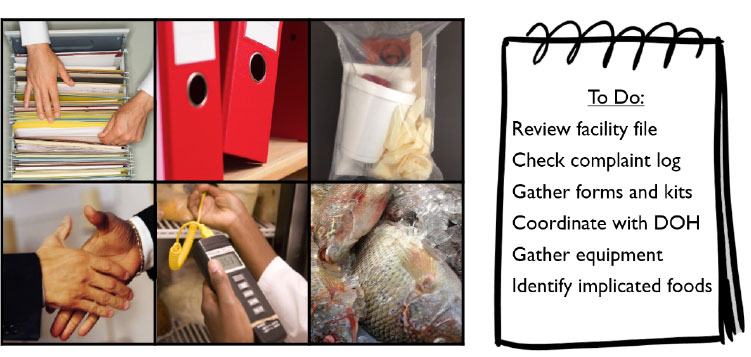
Conduct the inspection of the food establishment and collect food samples as soon as possible, but no later than 24 hours after notification of the possible foodborne illness outbreak. Be sure to plan the environmental investigation before arriving at the food establishment. The following items should be checked before leaving the office.
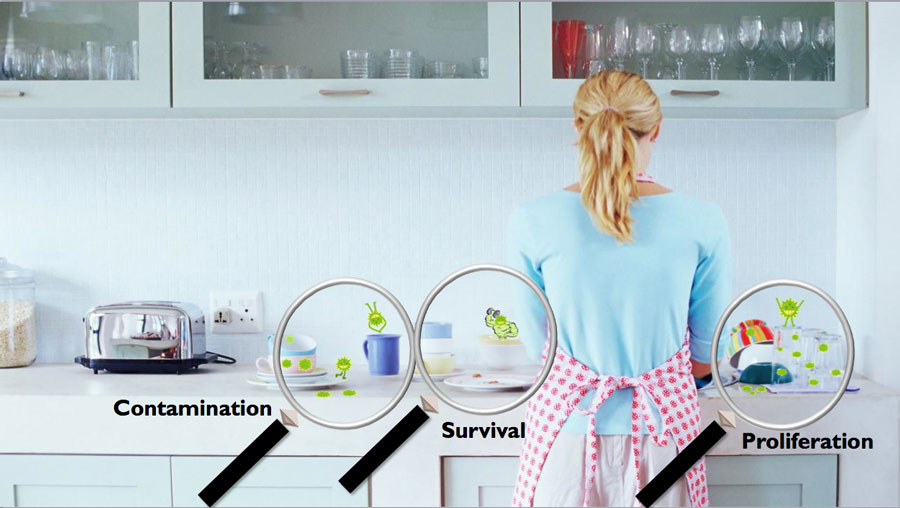
A full understanding of how microorganisms contaminate, survive, and proliferate within the environment is necessary to identify the association between foodborne illness and food handling practices.
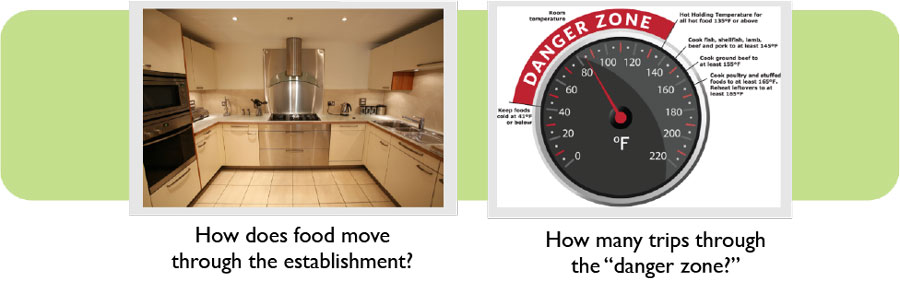
Understand how the food travels though the establishment and how that increases or decreases the likelihood of foodborne illness. Identify whether the food operations are simple or complex, that is, how many times the food passes though the temperature “danger zone” before it is served. Simple operations involve food preparation with no cooking or a single cooking step before food is served, while complex operations require multiple cooking, cooling, and heating steps. The more times a dish passes through the “danger zone” the more opportunity there is for microorganisms to grow and multiply.
Focus the investigation of the CDC Risk factors: Improper holding temperatures, inadequate cooking, contaminated equipment, food from unsafe sources, and poor personal hygiene.
Remember that the objective of the inspection is to ascertain the source and mode of microbial or chemical contamination of the food, the likelihood that pathogens survived processes designed to kill or reduce their numbers, and the opportunities for growth of pathogenic bacteria or toxigenic molds. With this in mind, be sure to maintain an unbiased, neutral attitude throughout the inspection.
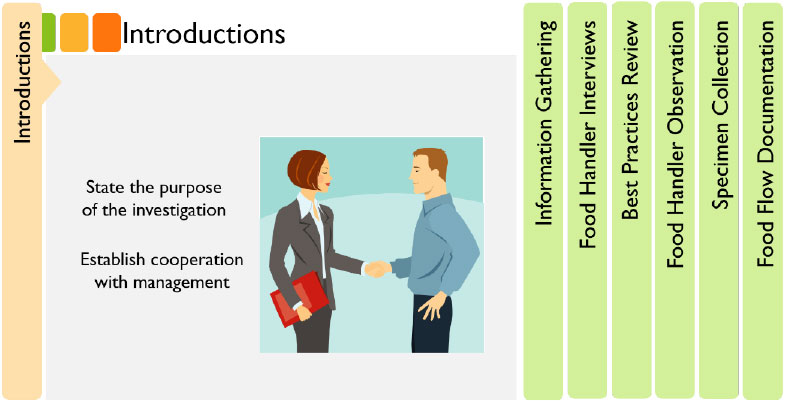
Introductions
Introduce yourself to the manager or person in charge on arrival at the food establishment. Begin by stating the purpose for the inspection. Try to establish a level of cooperation with management and assure them that every potential source of contamination will be investigated.
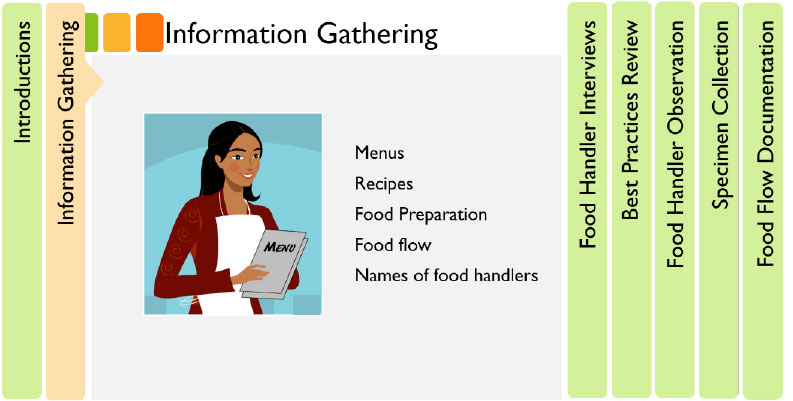
Information Gathering
Get information on menus, recipes, food preparation, food flow, names of food handlers, and their food handling responsibilities.
Food Handler Interviews
Interview the food handlers on their present and past health using the Food Handler Questionnaire.
Best Practices Review
Review food handling practices with food handlers. Concentrate on the preparation of those suspect foods previously identified including amounts, recipes, and sources of raw ingredients.
Food Handler Observation
Observe the food handling practices taking place while in the food establishment. Pay close attention to high risk foods, for example, those that are served raw or require extensive handling.
Specimen Collection
Collect leftover foods from the establishment for testing. If there is a suspect meal or food item, be sure samples of those items are collected as well. If no leftover foods are available, collect raw ingredients or similarly prepared foods. It is very important that the proper collection procedures are strictly followed, as improper collection could prevent adequate testing. Don’t forget that food samples should be accompanied by the chain of custody form. Before collecting samples, please review the sampling procedures outlined in Resource 10.10.4.
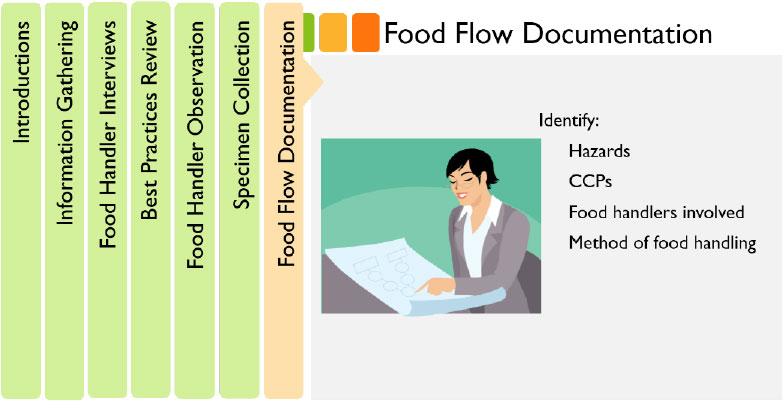
Food Flow Documentation
Draw a separate flow chart showing each operation that the suspect foods underwent. Identify the hazards, critical control points (CCPs), specific food handlers involved with the operation, and actual food handling practices involved. This approach may help to identify the breakdown in food handling that led to the foodborne illness. The flow charts may be revised repeatedly as new information is gathered.
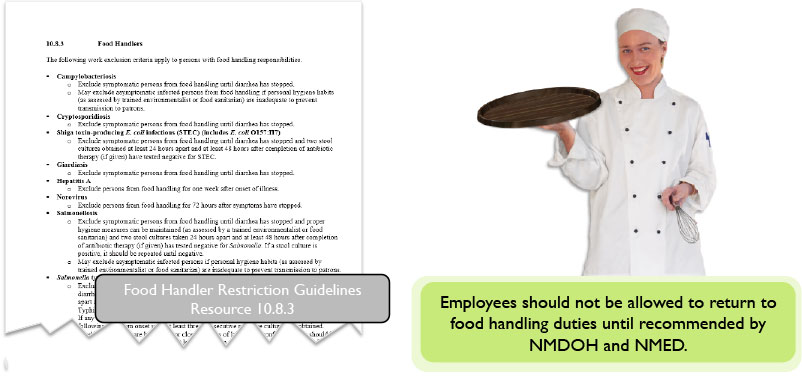
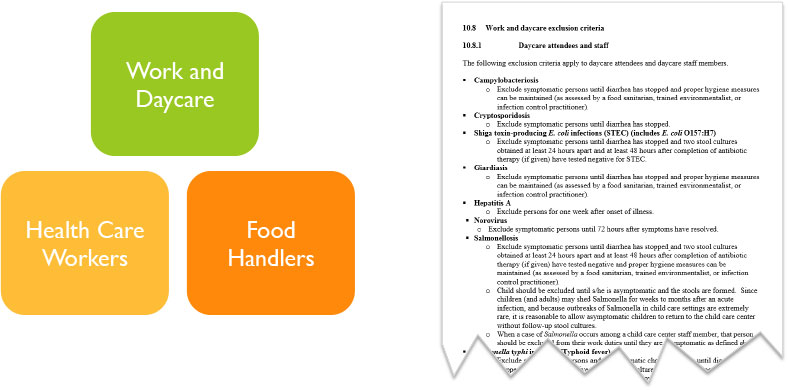
Persons should be excluded from food handling if diagnosed with any communicable disease that can be transmitted through food or if suffering symptoms of acute gastrointestinal illness including nausea, vomiting, or diarrhea. However, if the food handler can document that these symptoms are the result of a noninfectious condition such as Irritable Bowel syndrome (IBS) or during the early stages of a pregnancy, the food handler may remain working in a full capacity. Excluded employees should not be allowed to return to food handling duties until recommended by NMDOH and NMED. Refer to Section 10.8 for the exclusion criteria for specific foodborne illnesses.
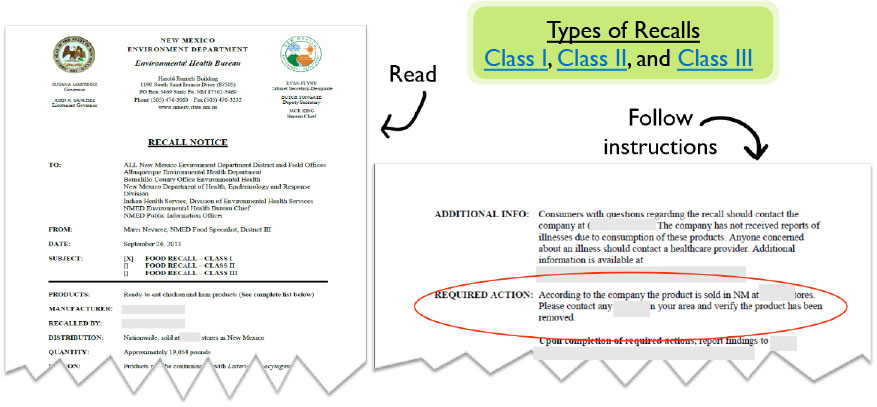
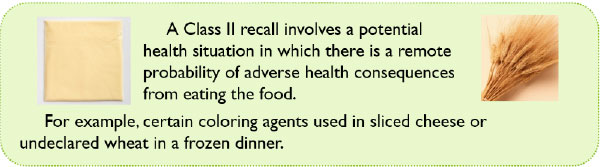
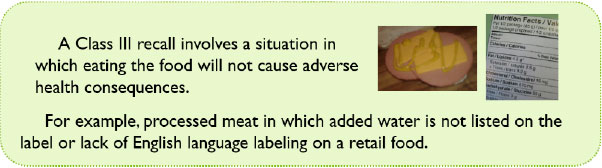
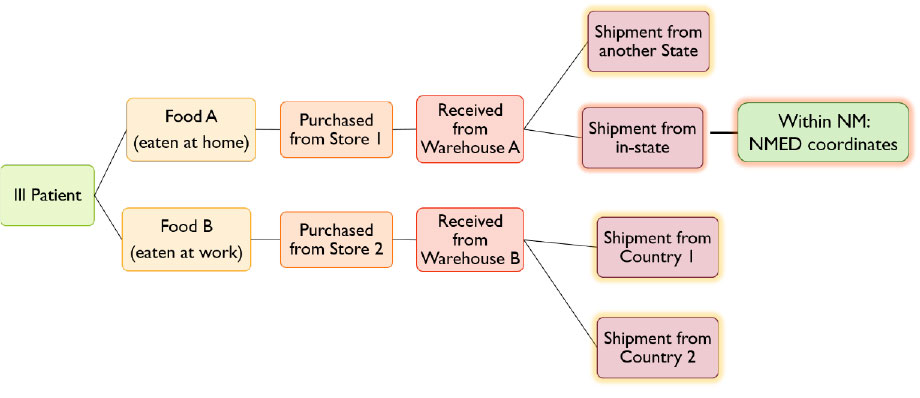
If the epidemiologic and environmental investigation findings indicate that a recall or traceback is necessary, coordinate with NMED, NMDOH, and other partners to complete these activities. A recall occurs when a product can potentially cause harm to the consumer. NMED issues a recall notice to ensure the product has been removed from circulation. Refer to Section 10.9 for a NMED Recall Notice template.
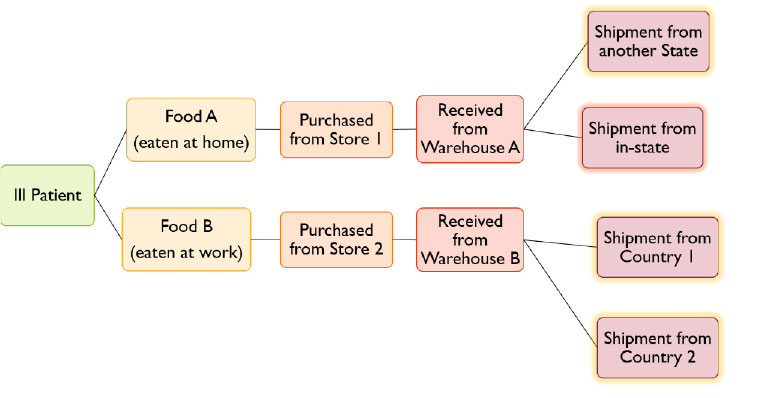
The purpose of a traceback is to follow the flow of a food product back to its original source. The steps in the process from the finished product to the farm ingredients used are investigated to identify the source of the product adulteration and/or product process break down.
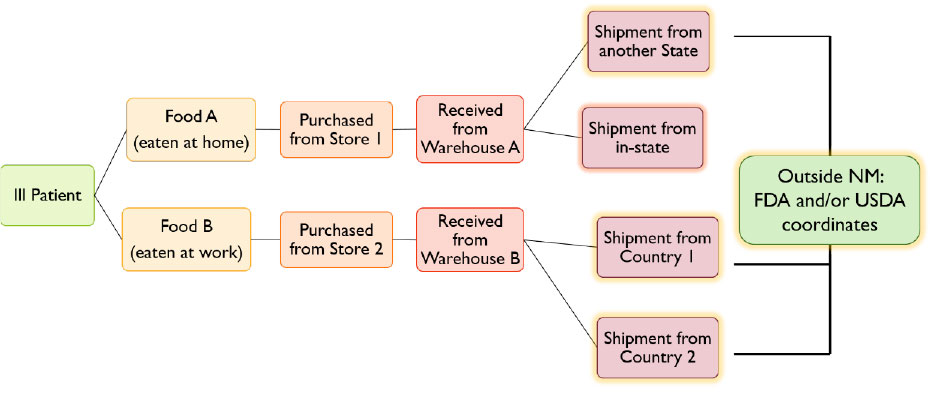
Traceback of food products processed outside of New Mexico are coordinated by FDA and/or USDA. The NMED Food Program Manager will act as a liaison with these Federal partners and coordinate New Mexico efforts in a traceback.
Traceback of food products processed within New Mexico will be coordinated by the regulatory agency that has jurisdiction over the food processor.
This module reviewed the components involved in the environmental investigation of a foodborne illness outbreak. Keep in mind that this module presents the response to a typical foodborne outbreak and there may be exceptions to the guidelines depending on the specifics of an investigation. When the epidemiologic and environmental investigations are completed, the investigation will be summarized in a final report. Continue to Module 6 to learn how to compile the final report and complete investigation follow up activities.
Module 6 references information from Chapters 7 and 8 in your manual. In this module you will learn all of follow-up actions that take place after an outbreak has ended. No outbreak investigation is truly over until these items have been completed.
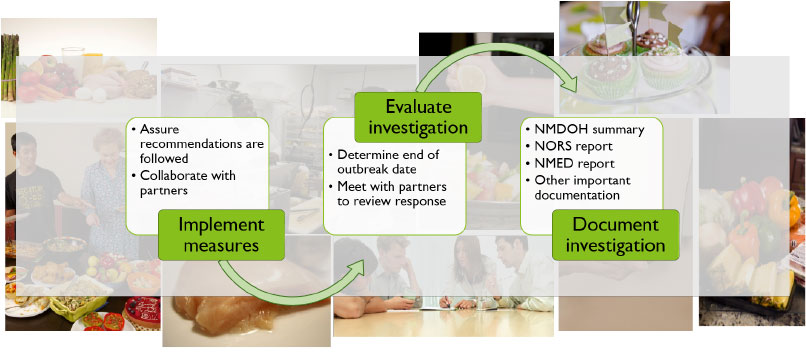
It is important to remember that a primary goal of the outbreak investigation is to prevent any ongoing risk to the public. Keeping that in mind, a key follow-up activity is assuring recommendations made to the establishment are followed, and remediation and prevention measures are implemented. It is also vital to evaluate the investigation process and determine the outbreak’s end date. One way to determine the outbreak end is when there have been no new cases from the last onset date to twice the incubation period of the implicated pathogen. Finally, detailed documentation of the investigation is the last step to complete outbreak follow-up. The remainder of this module will address the protocols surrounding adequate documentation. Remember that all members of the investigation team (including partner organizations) play an important role in each step of the follow-up process, and should be included wherever appropriate.
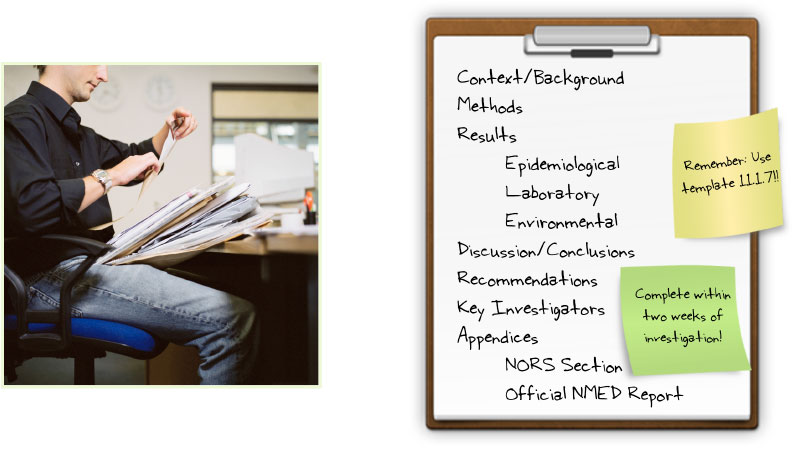
The outbreak investigation lead epidemiologist will prepare an archive folder and final written report summarizing the outbreak investigation within 2 weeks of investigation completion. The report should include all of these sections, if appropriate. A summary of any NMED environmental investigation findings should be included in the Environmental Investigation Results section of the final NMDOH written report. If available, a copy of the official environmental investigation report from NMED should be included as a Section. If a member of the outbreak investigation team other than the NMDOH lead epidemiologist completes the final written report, the report should be routed through the NMDOH lead epidemiologist for final approval and filing.
The final written report should be saved into the electronic NMDOH outbreak folder. The outbreak investigation number should be used to file electronic and hard copies of all documentation, including investigation notes. Electronic copies of documents associated with the investigation should be copied to the numbered outbreak folder.
The final NMDOH report should be distributed electronically to all of the appropriate stakeholders. The stakeholders will use the report during the close-out meeting.
The National Outbreak Reporting System (NORS) is a surveillance system maintained by the Centers for Disease Control and Prevention (CDC). State and local health departments in all states use NORS to electronically report data about foodborne outbreak investigations to CDC. These data are released by CDC in a public access database often used to evaluate state programs. NMDOH Foodborne Disease Epidemiologist has the primary responsibility for entering completed NORS reports into the CDC database.
A NORS report should be filed for each foodborne or waterborne outbreak investigation within 1-2 weeks of the completion of the investigation. Once the final outbreak report is completed, the Foodborne Disease Epidemiologist should be notified for NORS data entry. The NORS summary table in the final written investigation report template (Template 11.1.7) should be completed to facilitate NORS reporting. Additional information to be entered into NORS should be available in the outbreak final report.
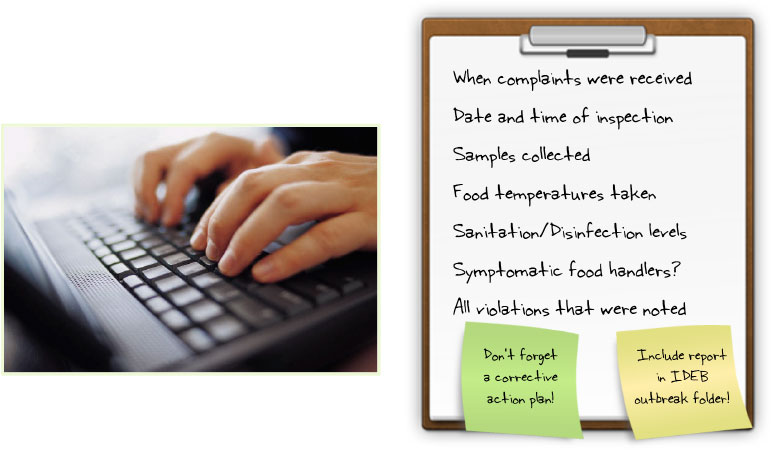
The goal of the NMED final report is to provide accurate and complete documentation about the establishment during the foodborne illness investigation. The NMED inspector(s) performing the investigation will prepare the final report, which should be restricted to actual inspection findings. All conclusions about suspected foods should be left to the IDEB final written report (see Section 7.1) and will be based on environmental samples, conditions in the facility, patient samples, and statistical analyses. A corrective action plan should be included that addresses deficiencies found during the inspection. The NMED report should be included in the outbreak archive folder.
In Module 6, we reviewed all of the follow up activities that occur after an outbreak investigation is completed. Although this may seem like a lot of work, each part of the process, from implementation of control measures to detailed documentation, are essential and should not be ignored or forgotten.
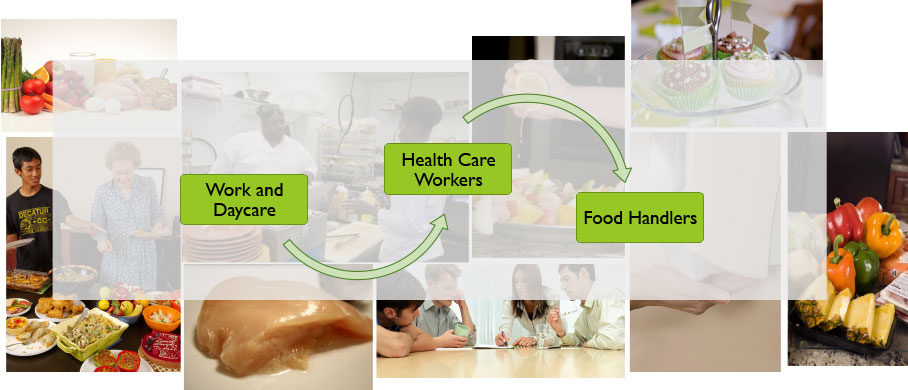
In this module we will review exclusion criteria through a series of multiple choice questions. For assistance, please reference Resource 10.8 in your manual.
Tessa was diagnosed with Giardia after spending the week at her grandparents' house in the mountains. She is currently symptomatic and not yet potty trained. Can she go back to daycare today?
No. She cannot return until diarrhea has stopped.
That's Correct!
No. She will need two negative tests, 24 hours apart.
I'm sorry, please try again.
Yes. As long as hygiene measures can be maintained.
Karen was diagnosed with Campylobacter two weeks ago. All of her symptoms have stopped and she did not care for patients while she was symptomatic. Can she return to work now?
Yes. Campylobacter is not a healthcare concern
I'm sorry, please try again.
No. She should be retested first
I'm sorry, please try again.
Yes. As long as her personal hygiene practices are adequate
That's Correct!
No. She should wait three weeks after symptoms stop
Christy (and Mr. Fluff) work at Christy's Kid Corral, a daycare center in Albuquerque. Christy has had vomiting and diarrhea since yesterday and is associated with a Norovirus outbreak currently being investigated. When do you recommend she return to work?
Dan's wife Julie contracted Typhoid fever after their mission trip to India. She is too sick to even think about work, but Dan feels just fine! He is cleared to provide patient care, right?
Yes. Dan is good to go!
I'm sorry, please try again.
Yes. But if he starts to feel sick he should stop
I'm sorry, please try again.
No. He needs to wait until his wife's symptoms resolve
One control measure that is essential to the outbreak investigation is the exclusion of symptomatic, and at times not asymptomatic cases. There are special criteria to follow depending on the case’s age or occupation. Keep in mind that you are not expected to memorize these criteria. The manual can be an extremely helpful reference as you work your way through all stages of an outbreak.
You have reached the end of this course. The next step is the final assessment.
Follow the 4 steps provided below to mark this course completed and to launch the Assessment.
Step 1 After you use the Close This Training button found at the bottom of this page to close this training, you will see the following screen, click on the Home button highlighted in blue found in the top left of the screen.
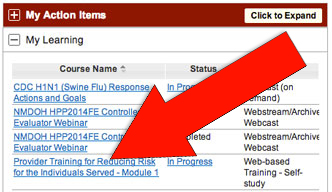
Step 2 From the Home sreen you will see your Dashboard on the right hand side of the screen, click on the My Learning tab and click on the course you just took which will be highlighted in blue.
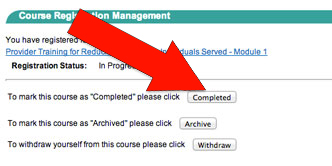
Step 3 Confirm that you have completed reviewing this course by clicking the Compelted button.
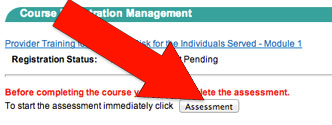
Step 4 The system will then prompt you to begin the quiz by clicking the Assessment button.









 Identify potential hazards and measures to control those hazards.
Identify potential hazards and measures to control those hazards. Critical Control Points: points in a food’s production at which the potential hazard can be controlled or eliminated.
Critical Control Points: points in a food’s production at which the potential hazard can be controlled or eliminated. Include critical limits for each control point.
Include critical limits for each control point. Monitor CCPs.
Monitor CCPs. Implement when monitoring shows that a critical limit has not been met.
Implement when monitoring shows that a critical limit has not been met. Verify that the system is working properly
Verify that the system is working properly Document the HACCP system.
Document the HACCP system.

 Perform data analyses as appropriate
Perform data analyses as appropriate





 Provide guidance and consultation regarding proper specimen handling and transport.
Provide guidance and consultation regarding proper specimen handling and transport.
 Report laboratory test results to PHD, IDEB, NMED, and private submitters and ensure involvement of all appropriate local agencies
Report laboratory test results to PHD, IDEB, NMED, and private submitters and ensure involvement of all appropriate local agencies












 Microorganisms
Microorganisms Food Flow
Food Flow Risk Factors
Risk Factors